12 |LES DÉFIS DE L'ATTEINTE DES OBJECTIFS DE DÉVELOPPEMENT DURABLE 3 ET 6 DANS L'ÉTABLISSEMENT INFORMEL DE DOUALA IV, RÉGION LITTORALE DU CAMEROUN
THE CHALLENGES OFACHIEVING SUSTAINABLE DEVELOPMENT GOALS 3 AND 6 IN THE INFORMAL SETTLEMENT OF DOUALA IV, LITTORAL REGION OF CAMEROON
Mots-clés:
Enjeux| Objectifs de Développement Durable| habitats informels| Douala IV|Résumé
Une grande proportion de citadins en Afrique subsaharienne réside dans des quartiers à habitats informels, connus pour leurs mauvaises conditions de vie et leurs problèmes de santé. De nombreuses personnes à Douala IV se sont installées dans des bidonvilles où l'accès à l'eau potable et à l'assainissement est assez difficile. Cela les expose à toutes sortes de maladies liées à l'hygiène et à l'assainissement et compromet la réalisation des objectifs 3 et 6 du Développement Durable (ODD). L'objectif de cette étude est d'analyser les défis à surmonter pour atteindre les ODD 3 et 6 dans les quartiers à habitats précaires de l’arrondissement de Douala IV. Pour y parvenir, nous avons adopté respectivement les approches quantitative et qualitative de recherche. Une technique d'échantillonnage aléatoire a été utilisée pour administrer 330 questionnaires à 22% de la population de cet arrondissement. Les résultats révèlent qu'il existe un problème d'accessibilité et de disponibilité de l'eau potable dans les quartiers à habitats précaires de l’arrondissement de Douala IV. Conséquemment, 78,8% de la population est abandonnée à elle-même en ce qui concerne l’accès à l'eau potable et, incidemment, les populations sont obligées de dépendre de l’eau issue des puits et forages généralement impropres à la consommation. Enfin, l’étude conclut que l’atteinte des ODD 3 et 6 dans ce contexte n’est pas envisageable. Par conséquent l’implication active des pouvoirs publics dans la planification urbaine et la mise à disposition des populations d’une eau de qualité et d’un système d’assainissement adéquat doivent être prioritaires.
Introduction
Ensuring sufficient availability of water for human and environmental needs is one of today’s most pressing global challenges. The demand for water for human consumption, sanitation, power, industry, agriculture and livestock, and other uses has accelerated more than twice as fast as the rate of population growth over the last century (United Nations, 2005; 2013). As a result, domestic water use has become the prime societal water need in both urban and rural areas. Household water supply has become an important public policy issue because safe water is mainly an essential component of primary health care. Access to improved water sources and sanitation is related to the health and survival of human capital (Mangyo, 2008; Tang et al., 2008; Mishra and Newhouse, 2009). Sub-Saharan Africa has been grappling with the issue of inadequate access to water and sanitation for decades (Sop, 2017). In the latest report, water comes after weapons of mass destruction, extreme weather events, and ahead of major natural disasters and climate change (World Economic Forum, 2018). The need to improve access to water and sanitation for men and women dates back to the 1977 United Nations Water Conference, the International Drinking Water and Sanitation Decade (1981-1990), the International Conference on Water and the Environment in Dublin (1992), also involved in the “Water for Life” decade (2005-2015), the Millennium Development Goals (MDGs), and The United Nations “2030 Agenda for Sustainable Development Goals”. In September 2015, the United Nations Summit on Sustainable Development adopted a new framework to guide development efforts between 2015 and 2030, entitled “Transforming Our World: the 2030 Agenda for Sustainable Development” (United Nations, 2015). This 2030 Agenda contains 17 Sustainable Development Goals (SDGs) and 169 targets (United Nations, 2015). These 17 SDGs are stated as follows: Goal 1: End poverty in all its forms everywhere; Goal 2: End hunger, ensure (achieve) food security and improved nutrition, and promote sustainable agriculture; Goal 3: Ensure healthy lives and promote well-being for all at all ages; Goal 4: Ensure inclusive and equitable quality education and promote lifelong learning opportunities for all; Goal 5: Ensure (achieve) gender equality and empower all women and girls; Goal 6: Ensure availability and sustainable management of water and sanitation for all; Goal 7: Ensure access to affordable, reliable, sustainable and modern energy for all; Goal 8: Promote sustained, inclusive and sustainable economic growth, full and productive employment and decent work for all; Goal 9: Build resilient infrastructure, promote inclusive and sustainable industrialization, and foster innovation; Goal 10: Reduce inequality within and among countries; Goal 11: Make cities and human settlements inclusive, safe, resilient, and sustainable; Goal 12: Ensure sustainable consumption and production patterns; Goal 13: Take urgent action to address (combat) climate change and its impacts; Goal 14: Conserve and sustainably use the oceans, seas, and marine resources for sustainable development; Goal 15: Protect, restore and promote sustainable use of terrestrial ecosystems, sustainably manage forests, combat desertification, and halt and reverse land degradation, and halt biodiversity loss; Goal 16: Promote peaceful and inclusive societies for sustainable development, provide access to justice for all and build effective, accountable, and inclusive institutions at all levels and Goal 17: Strengthen the means of implementation and revitalize the Global Partnership for Sustainable Development.
Nevertheless, the purpose of this study focused on Goals 3 and 6. It is important to notify that there is a close link between SDGs 3 and 6, for instance, poor hygiene and sanitation lead to poor health, and poor unsecured housing also leads to poor health. Thus, ensuring the success of one of these goals indirectly ensures the success of the other two (United Nations, 2015). SDG 3 is a multiple and universal resource on which sustainable development policies can build especially for countries that need it the most and can lead to the sustainable maintenance of well-being and health. However, SDG 3 faces a strong sectorization, so there is a risk of not being able to achieve the goals set. Health and wellness for all people are universal rights that, together with education, are arguably the best civilization tool to build harmonious, equitable, and just sustainable development (Guégan et al., 2018). In the same light, the establishment of SDG 6, to ensure the availability and sustainable management of water and sanitation for all, reflects the increased attention to water and sanitation issues on the global political agenda (UN-WATER, 2018). Nevertheless, UNICEF and WHO estimates that 1.1 billion people lack access to improved water supplies and 2.6 billion people lack adequate sanitation. Providing safe drinking water and basic sanitation to achieve the MDGs will require substantial economic resources, sustainable technological solutions, and courageous political will (Moe and Rheingans, 2006). According to the experts of the UNFPA (2004), population growth is one of the principal causes of the increase in the needs as regards housing, water, hygiene, energy, health care, education, social services, food, and difficulties of durable sanitation (Sadik, 1994). In urban areas, especially in informal settlements, the provision of adequate water and sanitation services is extremely difficult in poor countries. Unsafe water and poor sanitation are major causes of morbidity and mortality, especially among young children living in poor urban informal settlements. Many people living in informal settlements are unable to maintain adequate domestic hygiene or are unaware of health risks. Sanitation issues (such as the lack of proper waste disposal methods) are the cause of dozens of deadly contagious diseases, many of which are particularly prevalent among children, where running water and sewage systems are often limited and garbage collection is rare. These conditions do not only affect the people who live there; their effects also influence the rest of the city.
Although rich in natural resources, Cameroon lags behind the rest of the world on several indicators of social well-being. According to the 2016 Human Development Index (HDI) report published by the United Nations Development Program (UNDP), Cameroon falls into the category of low human development countries in the world. Indeed, the country is ranked 153rdin the world, out of 188 countries surveyed, and 23rdin Africa. More than half of the population suffers from poverty, including poor education and health, and a low standard of living.
Douala IV, the economic capital of Cameroon, attracts many people, including young people from all parts of the country and neighboring countries, in search of better opportunities. This has resulted in significant population growth, with an estimated average annual population growth rate of 5% over the past 30 years, well above the national rate of 2.8%. At this rate, the population of Douala IV is expected to triple by 2035. Low levels of access to sanitation coupled with high vulnerability to flooding pose enormous health risks to the population of Douala IV (Sop, 2017). In Douala IV informal settlements, unclean water, poor hygiene, and sanitation are major causes of morbidity and mortality mostly among children. Based on the issues raised above, the research question for this study is: what are the challenges to achieving SDGs 3 and 6 in the informal settlement of Douala IV?
Méthodologie
1. Materials and methods
1.1. Location of the study area
Located in the inter-tropical zone in the Gulf of Guinea in the Wouri estuary between latitudes 04°03’ and 04°9’ north and longitudes 09°34’ and 9°45’ east, Douala IV enjoys a humid tropical climate. Annual rainfall is over 4,000 mm, characterized by wet and dry seasons with temperatures ranging between 24 and 27°C. Douala IV is bordered to the north by the Mungo and Nkam divisions, to the east by Douala IV I, to the south by the Atlantic Ocean, and to the west by the South West Region of Cameroon.
Map 1: Geographic location of the study area
Source: Fieldwork, 2020
1.2. Data collection and management
This study used a descriptive research design; it attempts to establish a cause-and-effect relationship among the variables used in this research. Data were obtained through questionnaires administered to the population of Nyalla, New-Bell, and Boanangang to obtain information on their opinions regarding the challenges they face in their communities concerning achieving SDGs 3, and 6. In-depth interviews were conducted with the relevant authorities in charge of urban planning in Douala IV. Data on the health of the population were also obtained from four health institutions: the first in Boanangang, the second in Nyalla, and the third and fourth in New Bell. Water samples were collected from household wells and analyzed at the laboratory of the Wastewater Research Unit of the Faculty of Science of the University of Yaoundé I to assess water quality in the informal settlement of Douala IV. To determine the sample size for each quarter, a certain percentage of respondents was obtained from the 261,407 (Douala IV) plus 646,347 (Douala IV) and 544,019 (Douala IV) for a total of 1,452,673 people. 10% of the target population was the sample size used for this research. Therefore, the sample size = 0.1x 1,452,673= 145,267.3. Using a random sampling technique, 330 questionnaires were administered to the target population living in the selected area in an informal settlement in Douala IV. The collected data were entered into a spreadsheet using the Statistical Package for the Social Sciences (SPSS) version 21. Both descriptive and inferential statistical methods were employed in this analysis.
1.3. Ethical approval
The protocol for this study was independently reviewed and approved by the University of Bamenda Ethics Committee. Informed consent was obtained from all participants included in the analysis. They were then invited to voluntarily participate in this research. They were informed that the study was confidential and that their participation will not affect their care. The agreement was materialized by the signing of the informed consent form.
Résultats
2. Results
2.1. Physical accessibility to the health institution in the informal settlement of Douala IV
Goal 3 of the UN SDGs is to ensure healthy lives and promote well-being for all of all ages. The target of item 3.4 of SDG 3 by 2030 is to reduce premature mortality from non-communicable diseases by one-third through prevention and treatment and to promote mental health and well-being. Achieving the goal of good health and well-being in urban areas of poor countries appears to face serious challenges. In the informal settlement of Douala IV, the challenge seems greater due to the level of poverty of its population.
The proximity of health facilities is a great advantage for the health of the population. Closeness to the health institution will significantly reduce the death rate, lower the cost of going to a health center, and motivate people to go to the hospital when they are sick. Map 2 presents the physical accessibility to healthcare units in the study area.
Map 2: Accessibility to healthcare institutions in the informal settlement of Douala IV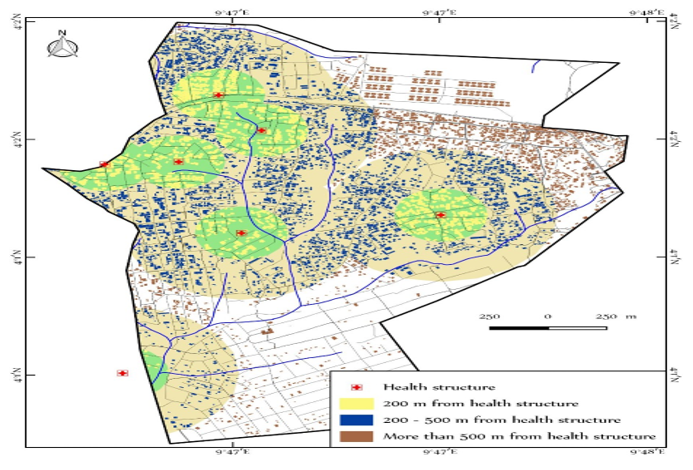
Source: Fieldwork, 2020
According to map 2, most residents of the informal settlement of Douala IV travel more than half a kilometer (500m) before reaching health institutions. This constitutes a restriction to the dimension of healthcare accessibility based on physical distance. The health facilities located at the shortest distance (200m) are those of low quality and the population’s demand is greater than the availability of these services in these facilities. This difficulty of distance given the high doctor-to-patient ratio is a constraint to achieving the healthcare-related SDGs by 2030.
2.2. Staying away (abstention) from healthcare facilities and self-medication
People react differently to health problems depending on their financial capacity. In the informal settlement of Douala IV, some people resort to self-medication, and others turn to the hospital when they have a health problem, each according to their financial power. But the vast majority turn to the hospital when the health situation is critical. Moreover, many people are responsible for their hospital bills; very few have health assurance because very few are government workers (civil servants). The field report shows that more than half of the population has had a case of illness in their home in the last three months. 51% of the population agrees that either they or someone in their household has felt sick in the last three months and 49% disagree. People use a variety of means to care for themselves when they are sick. Table 1 presents the reality of the informal settlement in Douala IV.
Table 1: Methods of treatment by respondents in an informal settlement of Douala IV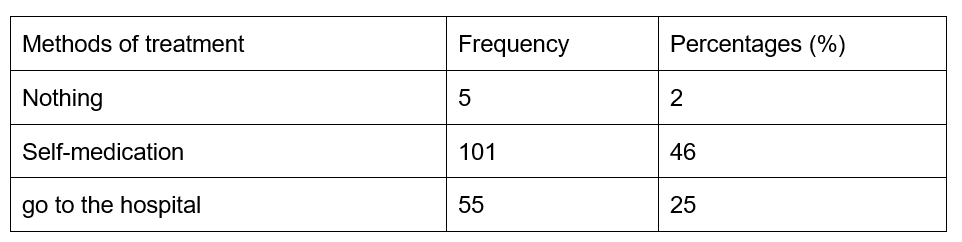
Source: Fieldwork, (2020)
When faced with illness, 2% of the people do nothing when they are sick, 46% treat themselves (self-medication), 25% go to the hospital, and 26% turn to other means, like visits to native doctors or herbalists. The percentage of those who go to the hospital is really low, which means that the health situation of the population in the informal settlement of Douala IV is in danger, and if nothing is done, SDG3 will not be achieved here by 2030. Among the poor, many people often take the time to observe the patient for two or three days before taking him to the hospital, due to lack of money. In the informal settlement of Douala IV, many people take their patients to the hospital when the case is bigger than theirs. Table 2 shows how people in the informal settlement of Douala IV behave in case of illness. Field statistics reveal that 29% of respondents go to the hospital at the very beginning of the illness, 21% when the illness is not yet too severe, 41% when the illness is severe, and 9% go to the hospital when the illness is very severe. So, in general, people always try to manage the patient at home and refer him to the hospital when the case is out of control. In the commune (municipality) of Douala IV, people have various reasons for not doing anything to treat themselves when they are sick. But at the heart of all these reasons is the lack of money (table 2).
Table 2: Reason why people don’t do anything to treat themselves when they are sick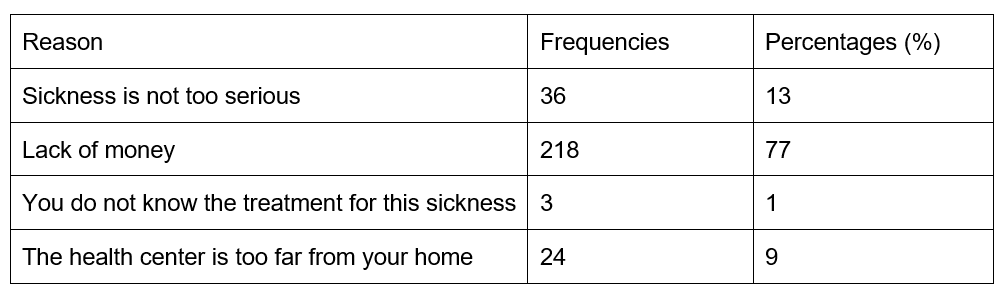
Source: Fieldwork, (2020)
According to table 2, 13% answered that it is because the illness is not too serious, 77% said it is because of lack of money, 1% answered that they do not know what to do, and 9% that the health center is too far. Lack of money is therefore the main reason why people do nothing to treat themselves when they are sick in the informal settlement of Douala IV. The SDGs are far from being achieved in the informal settlement of Douala IV considering this indicator.
Most people choose to self-medicate in the informal settlement of Douala IV. Self-medication is the primary means of treatment that people turn to in the context of poverty. It is cheap and available because it is done through the use of grass or the backs of trees. Table 3 reveals the reason why people choose self-medication in the informal settlement of Douala IV.
Table 3: Reasons why people choose self-medication in the informal settlement of Douala IV
Source: Fieldwork, (2020)
Table 3 reveals that 76% of the population said they choose self-medication because of lack of money, 19% said because it is cheap, and 5% gave the distance to the health facility as the reason for choosing self-medication. The Cameroonian government has banned the practice of buying medicine at the roadside. But in the informal settlement of Douala IV, people are far from this reality (Table 4).
Table 4: Places where the population buys their drugs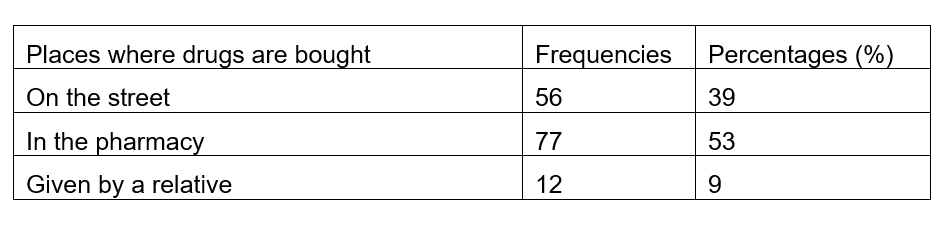
Source: Fieldwork, (2020)
Table 4 shows that 39% of the inhabitants of the informal settlement of Douala IV buy their medicines in the streets, 53% in pharmacies and9% were given by relatives. Although the percentage of those who purchase medicines in Pharmacies is encouraging, a good number of people (39%) continue to buy them on the street, which is dangerous for their health.
2.3. Water sources in the informal settlement of Douala IV
In the informal settlement of Douala IV municipality, people collect water from different sources and for various uses. Some collect water from taps, wells, springs, or boreholes, which are often privately owned (figure 1). In this commune, the population, often poor, relies primarily on well water for domestic use. They struggle to buy water from borehole owners to drink, with 20 liters costing 50 CFA francs. The price alone shows that water is not at the level of the common man, so they use the well water for their domestic work and only buy the water they are going to drink.
Figure 1: Water sources in the informal settlement of Douala IV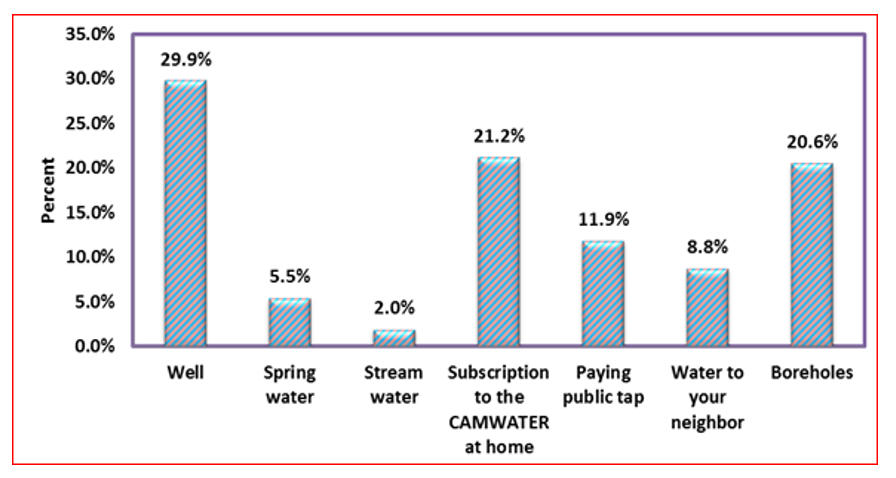
Source: Fieldwork, 2020
The results show that 29.9% of the population in the study area obtains its water from wells, 5.5% from springs, 2.0% from streams, 21.2% subscribes to Cameroon Water Utilities Corporation (CAMWATER) at home, 11.9% rely on public taps for their water consumption, 8.8% fetch water from their neighbors, and 20.6% rely on water from boreholes. Less population in the informal settlement of Douala IV is connected to CAMWATER. Generally speaking, CAMWATER is supposed to be the most reliable source of water for consumption that is not harmful to the health of the population. But if what is good for the health of the population is not available at all or is limited to a selected few, the rest of the population will be forced to turn to what is available and, in so doing, expose themselves to all kinds of diseases. Wells are the main source of water supply for the population in the study area. These boreholes (wells) vary in quality as shown in plate 1.
Plate 1: Differences in borehole quality in the informal settlement of Douala IV  Source: Fieldwork (2020)
Source: Fieldwork (2020)
The population in the informal settlement of Douala IV is at risk if nothing is done to improve their access to a safe water source. The fact that the largest source of water in the informal settlement of Douala IV is a well rather than taps, which have a high level of sanitation; is evidence that the population has poorer and unsustainable water sources. This has further exposed the population to water-borne diseases. All of this has led to challenges in achieving the SDGs related to accessibility to safe drinking water, healthcare, and safe cities. Based on this analysis, the study area is not safe and resilient, which poses a challenge for SDG 6.
2.4. Water accessibility in the informal settlement of Douala IV
The challenges to achieving the SDGs are very significant with water accessibility in the informal settlement of Douala IV. Water accessibility is the ease with which water can be obtained from the various sources in the area. It is considered in terms of dimensions of water accessibility, such as physical, economic, and social accessibility, as presented in Table 5.
Table 5: Dimensions and indicators of water accessibility in the informal settlement of Douala IV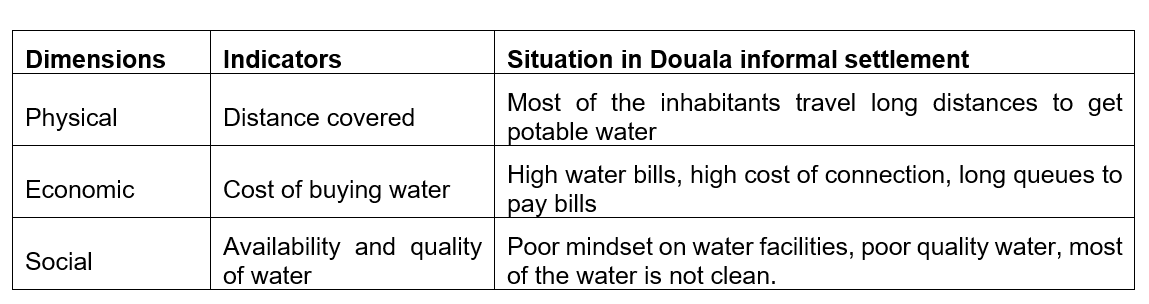
Source: Fieldwork, (2020)
The results in Table 5 show that with all dimensions of water accessibility in the study area, the indicators were not met. Most of the applicable indicators in the informal settlement of Douala IV show that there is a dismal high performance in the achievement and attainment of water accessibility indicators in the study area. Field data indicate that the distance between the house and the water collection point is a major challenge in achieving SDG 6 in Douala IV (Table6).
Table 6: Distance covered between homes and water collection point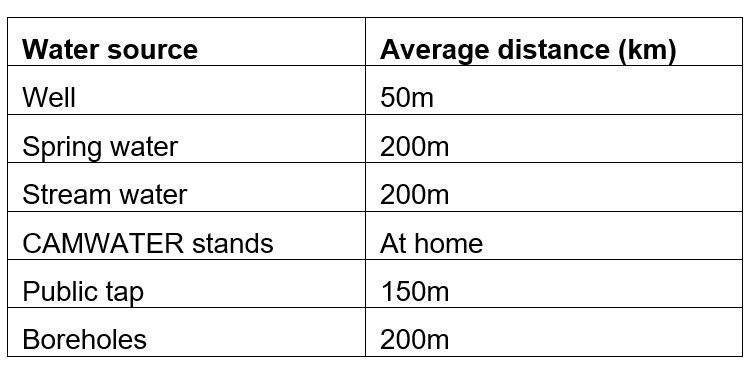
Source: Fieldwork, (2020)
Table 6 shows that people do not have direct physical access to water in the study area. People travel to other locations far from their homes to obtain water. This aspect of physical accessibility, which is distance shows that since the inhabitants do not have water at home, SDG 6 is far from being achieved. According to the population, 49% of the inhabitants walk and cover long distances to obtain drinking water. CAMWATER is the best and safest source of water after an investigation in the study area. Also, 61% of the respondents in the informal settlement of Douala IV do not have drinking water available in their homes. This challenge is based on the fact that the water supply actors are not able to respond to the water supply given the uncontrolled population growth and housing expansion in the informal settlement of Douala IV. The study, therefore, predicts that this limited access to water is already a challenge to SDG 6, which may not be met by 2030. The study determined the number of people connected to CAMWATER standpipes and made projections as shown in Table 7.
Table 7: Distribution of the number of people connected to CAMWATER in the informal settlement of Douala IV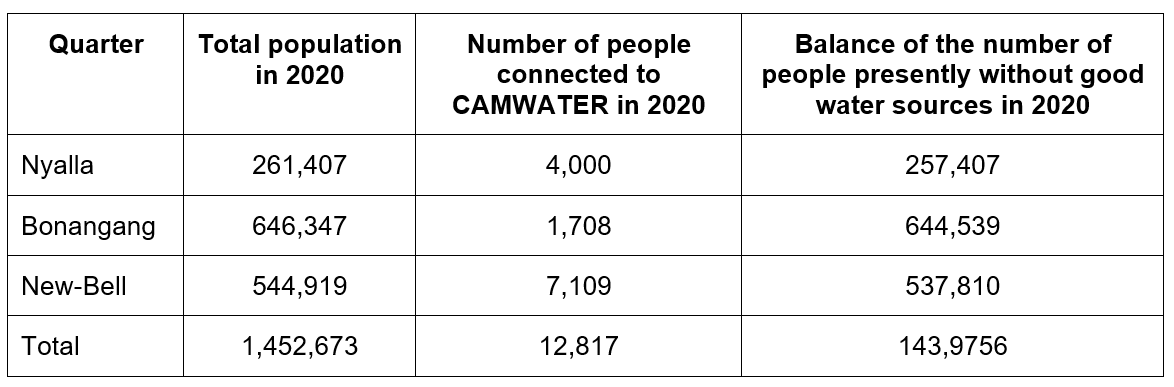
Source: Calculations projected from CAMWATER statistics (2020)
Based on table 7, the population of the study area is disproportionately larger than the number of people with the most preferable quality water source in the study area.
The population projection in 2030, was made using the formula Po=P1 (GR+1) n, where Po=current population, P1= previous population, GR= growth rate, and n= number of years. Thus, the projected population in 2030 will be 1,588,478, and projecting the number of people who will be connected to good water sources by 2030 stands at 17,943 individuals. Therefore, 1,581,046 citizens of Douala IV will not subscribe to CAMWATER, compared to 1,447,365 people in 2020 in this area, 2030. This means that 135,805 people will have been added to the population in2030. Insufficient water exposes people to dirt and therefore to diseases. This distance challenge, if not addressed, will be a challenge to achieving the SDGs.
2.5. Water quality in Douala IV
Table 8 shows the results of laboratory analyses of the physicochemical parameters of water from wells and boreholes in the area of study.
Table 8: Physicochemical and bacteriological analysis of boreholes and well water in the study area (Douala IV)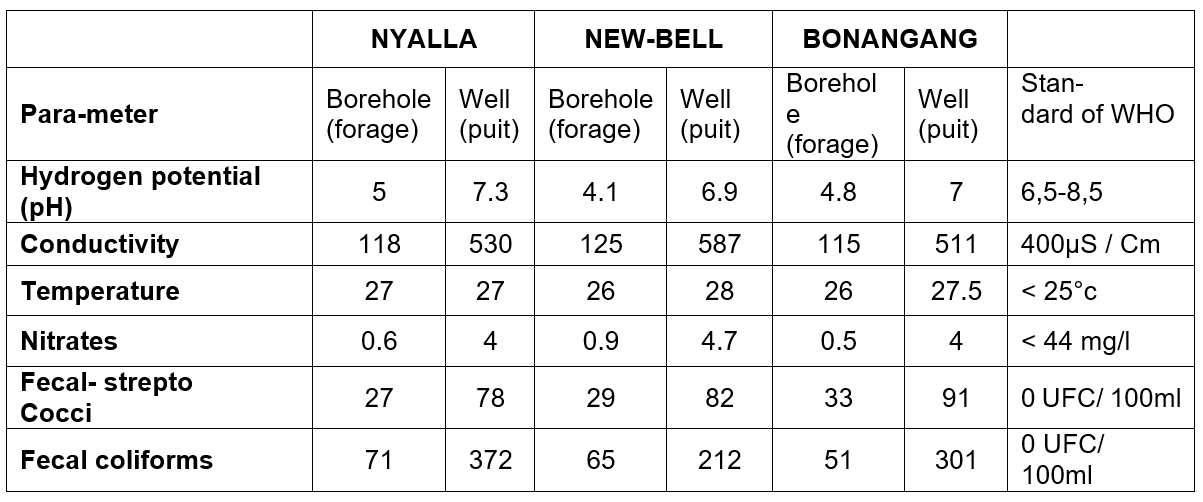
Source: Fieldwork, (2020)
From the above table 8, it can be seen that according to WHO (2005), the normal hydrogen potential (pH) is 6.5 and 8.5, water conductivity is 400µm, temperature < 25°C, water nitrate <44mg/l, fecal streptococcus 0 UFC/100 ml, and fecalcoliform0UFC/100 ml.
The temperature values of the sampled water are between 26 and 28°C. They do not comply with WHO (2005) standards, which recommend a temperature below 25°C for drinking water.
The physicochemical lab results (Table 8) show that the PH of the analyzed water points from the well respects the standard set by WHO (2005), which is 6.5 to 8.5, while the water from the boreholes does not. Conductivity is proportional to the degree of mineralization and varies according to temperature: it is more important when the temperature increases. Conductivity, as such, has no direct effect on health, as it reflects all the dissolved minerals. Mineralization can lead to a salty taste in some cases. However, conductivity is one of the means of validating physicochemical analyzes.
In the areas studied in the city of Douala IV, the conductivity values of the water from the Nyalla, New-Bell, Kassalafan, and Bonamoussadi boreholes meet the standards recommended by WHO and the EU (400µS/Cm). Conductivity values for these wells range from 115 to 125µS/Cm. However, the wells sampled at New Bell (Kassalafan), Nyalla, and Bonamoussadi (Bonangang) have conductivity values between 511 and 587 µS/Cm. The ingestion of nitrate is a potential risk factor for human health. They are present in surface water at a rate of 0.03 to 1 mg/l. At the end of the treatment facilities, their value must be lower than 0.1 mg/l. For drinking water, the accepted quality limit is between 50 and 100 mg/l, except for pregnant women and infants. The ingestion of nitrates in high doses is likely, under certain conditions, to disrupt blood oxygenation in infants. Moreover, they are suspected of participating in the development of digestive cancers. Above 100 mg/l, water should not be consumed. These salts are transformed in the body into nitric acid (HNO3). These reactions are due to the difference between the pH of the natural environment (water) and the pH of the body. The results also indicate the presence of nitrates without danger for the populations in the water of the analyzed boreholes and wells because their contents are well lower than the standards recommended by WHO (<44 mg/l). These nitrates come from the decomposition of organic matter, notably from the uncontrolled discharge of solid waste.
Also, the water from the wells and boreholes studied has an unevenly high concentration of fecal streptococci. The mere presence of fecal coliforms and fecal streptococci in the water automatically makes it unfit for human consumption according to the drinking water standards recommended by the WHO. By deduction, they contaminate the water of wells and springs used by the populations by the phenomenon of leaching of pathogenic germs and pollutants coming from the innumerable surrounding waste. Factors explaining the spatial differentiation of results include the geographical position of water points (plain, mid-slope, and summit), the density of the built environment, the level of maintenance of water points, and the presence of various types of waste, etc.
2.6. Hygiene and sanitation in the informal settlement of Douala IV
The hygiene and sanitation situation in the informal settlement of Douala IV is often very poor due to the unplanned growth of the population. The population faces daily poor waste management and a lack to access to public toilets.
2.7. Waste management in the informal settlement of Douala IV
As an urban area grows, so does the amount of waste. People eat every day and must have some way to dispose of their waste. But waste management is quite poor in urban centers and even worse in informal settlements. In the informal settlement, no planning has been done and no means of waste disposal has been provided, so everyone does their best to get rid of their waste. In planned urban centers, the government places public garbage cans at the roadside to facilitate waste management. In the informal settlement of Douala IV, people often rely on Hygiène et Salubrité du Cameroun (HYSACAM) to come by once or twice a week. When it is not available, people develop other means to dispose of their waste. This situation reveals the fact that in the informal settlement of Douala IV, hygiene and sanitation conditions are poor. Plate 2 shows the poorly disposed waste piles in the study area.
Plate 2: Piles of improperly disposed waste in the informal settlement of Douala IV
Source: Fieldwork, (2020)
A and B: waste dumped along houses and D waste dumped in the gutter and rivers. Photos C and D. This is a major challenge for SGDs because waste disposal and management are still weak in this area.
2.8. Types of toilets in different households in the informal settlement of Douala IV
The type of toilet reveals the socio-economic condition of the people. When people are financially viable, they often build their houses with modern toilets. But when financial means are limited, they build traditional toilets. For those who can afford it, they build both types of toilets, mainly to solve the problem of the water crisis. In the informal settlement of Douala IV, a large number of people often have traditional toilets (Table 9).
Table 9: Category of toilets in the different homes in the informal settlement of Douala IV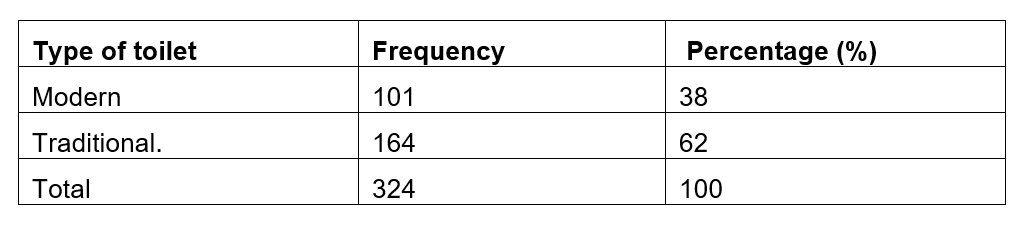
Source: Fieldwork, 2020
According to table 9, 38% of respondents have modern toilets in their homes, while 62% have traditional toilets. The spread of communicable diseases is easier when people share toilets with others. It is limited to cases where people use their toilets alone. But poverty forces some people in the informal settlement of Douala IV to build one toilet to be used by all their tenants. Thus, 10 or 20 people may share the same toilet and even the same bucket. 35% of the inhabitants of the informal settlement of Douala IV share their toilets with their neighbors, compared to 65% who do not. This effect is high and may promote the spread of diseases among the population of the informal settlement of Douala IV. Many people in the informal settlement of Douala IV share their toilets with a large number of people (Figure 2).
Figure 2: Number of people sharing toilet
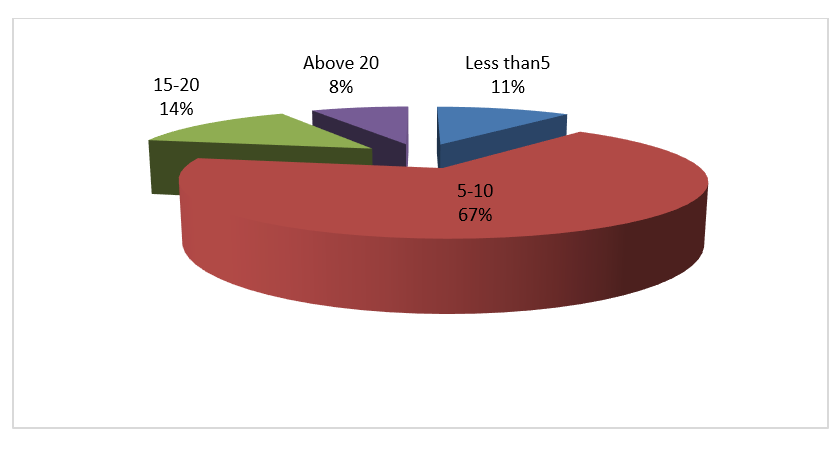
Source: Fieldwork, 2020
According to figure 2, 4,11% of people share a toilet with 5-10 people, 67% share with 10-15 people, 14% share with 15-20 people, and finally, 8% share with more than 20 people. These results show that the hygiene conditions in the informal settlement of Douala IV are really bad. Many more people are exposed to contagious diseases.
Conclusion
This study shows that there is a problem with water accessibility, water availability, water quality, and water management in the informal settlement of Douala IV, forcing the population to rely on well water, spring water, and borehole water. It was revealed that most residents of the informal settlement of Douala IV travel more than half a kilometer (500m) before reaching health institutions, which constitutes a restriction to the dimension of healthcare accessibility based on physical distance. Therefore, Self-medication is the primary means of treatment that people turn to in the context of restriction to the dimension of healthcare accessibility and poverty. It resulted also from the physiochemical and bacteriological analyses of water quality used by household in Douala IV are below the standards set by WHO which are not good for their health. The state of hygiene in the study area is also challenging. Therefore, to achieve the sustainable development goals 3 and 6 in the informal settlement of Douala IV, the government’s planning of informal settlement and provision of water, infrastructure, and health services should include the population and involve them in all development plans from conception design to implementation.
Références
Bibliographical references
ASSAKO ASSAKO René Joly, 2005, « Problématique de l’estimation de la qualité de vie dans un front d’urbanisation en Afrique : le cas du Bois des Singes à Douala (Cameroun) ». In Bley D. (éd.) : Cadre de vie et travail : les dimensions d’une qualité de vie au quotidien, Éditions Edisud : 65-85.
ASSAKO René Joly, MEVA’A ABOMO Dominique., TCHUIKOUA Louis Bernard, 2005, « Étude géographique de l’épidémie de choléra à Douala ou la qualité de vie à l’épreuve des pratiques urbaines ». In Fleuret S. (dir.) : Espaces, qualité de vie et bien-être, Presses Universitaires d’Angers, Angers : 307-315.
DJUISSI TEKAM Dorine, VOGUE Noel, NGWAYU NKFUSAI Claude, EBODE ELA Maurice, NAMBILE Cumber, 2019, “Access to safe drinking water and sanitation: a case study at the district community, in Douala V (Cameroon)”, the African Field Epidemiology Network, Pan African Medical Journal, ISSN: 1937- 8688. doi:10.11604/pamj.2019.33.244.17974.
GUÉGAN Jean-françois, SUZAN Gerardo, KATI-COULIBALY Séraphin, BOUPAMGUE Didier NKOKO, Moatti Jean-Paul., 2018, “Sustainable Development Goal 3, “health and well-being”, and the need for more integrative thinking”. Veterinaria México OA. 2018; 5(2). Doi:10.21753/vmoa.5.2.443.
MANGYO Eiji., 2008, “The effect of water accessibility on child health in China”. Journal of Health Economics, 27, 1343-1356. http://dx.doi.org/10.1016/j.jhealeco.2008.04.004.
MISHRA PRACHI., Newhouse David, 2009, “Does health aid matter?” Journal of Health Economics, 28, 855-872. http://dx.doi.org/10.1016/j.jhealeco.2009.05.004
MOE Christine L, RHEINGANS Richard D. 2006, “Global challenges in water, sanitation and health”, J Water health, 41-57p, http://dx.doi.org/10.2166/whj.2006.0043
SADIK NAFIS, 1994, Etat de la population mondiale. Choix et responsabilités. FNUAP, 78 p.
SOP SOP Maturin Desire (2017): “Taking Knowledge into practice”. LIRA Project, 17p. Unpublished
TANG KAM, CHIN Jackie, RAO PRASADA, 2008, “Avoidable mortality risks and measurement of wellbeing and inequality”. Journal of Health Economics, 27, 624-641.
United Nations, 2013, Water scarcity. http://www.unwater.org/statistics/thematic-factsheets/en
WHO Regional Office for Africa, 2012, Child and Adolescent Health. http://www.afro.who.int/en/clustersa-programmes/frh/child-and adolescent/Feb 2020
United Nations, 2015, Transforming our world: the 2030 Agenda for Sustainable Development, Resolution adopted by the General Assembly on the 25 September 2015, New York, 35p.
UN, 2018, Water Annual Report, 44p.
World Economic Forum, 2018, Annual Report 2017-2018, Cologny/Geneva p.96.

Downloads
Publié
30/06/2022
Comment citer
Revue Espace, Territoires, Sociétés et Santé ,[En ligne], 2022,, mis en ligne le 30/06/2022. Consulté le . URL: https://retssa-ci.com/index.php?page=detail&k=259
Numéro
Rubrique
Qui sommes-nous ?
Licence
Copyright (c) 2023 SOP SOP Maturin Désiré, MBEUTCHA Anmik Josiane et KEMADJOU Mbakemi Deric Larey

